Current role of ultrasound in hemodialysis access evaluation
Meola Mario , Jose Ibeas and Jan Malik
Abstract
JVA The Journal of Vascular Access
Physical examination (PE) is considered the backbone before vascular access (VA) placement, during maturation period and for follow-up. However, it may be inadequate in identifying suitable vasculature, mainly in comorbid patients, or in detecting complications. This review highlights the advantages of ultrasound imaging to manage VA before placement, during maturation and follow-up. Furthermore, it analyses the future perspectives in evaluating early and late VA complications thank to the availability of multiparametric platforms, point of care of ultrasound, and portable/ wireless systems. Technical improvements and low-cost systems should favor the widespread ultrasound-based VA surveillance programs. This significant turning point needs an adequate training of nephrologists and dialysis nurses and the standardization of exams, parameters, and procedures.
Keywords
Vascular access, B-Mode and pulsed wave Doppler, vascular access surveillance, ultrasound instrumentation, point of care of ultrasound
Date received: 7 January 2020; accepted: 5 July 2021
Introduction
Correct management of native arteriovenous fistula (AVF) or arteriovenous grafts requires specific knowledge and expertise and a multidisciplinary team approach. Early referral of uremic patients to a nephrologist—usually con- sidered the vascular access (VA) coordinator—is the main- stay to increase fistula placement, to ensure a correct and multidisciplinary approach, reduce the primary failure rate, and improve the cumulative VA patency.1
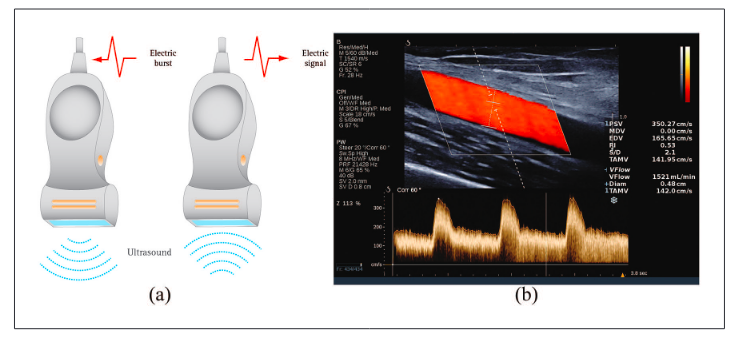
Before VA creation, patients’ presurgical assessment has been based on physical examination (PE) for a long time, and phlebography was the gold-standard imaging.2,3 Currently, ultrasound (US) and pulsed wave Doppler (PWD) are the first-line imaging for VA management.4–6 Safety, availability, and reliability are the main advantages of ultrasound modalities.
Therefore, non-invasive imaging impact has remarka- bly increased in the last years because most AVF with an inflow or outflow stenosis can be treated with percutane- ous transluminal angioplasty (PTA) to increase long-term survival.2,7 Meanwhile, US platforms have dramatically improved since the 1990s, when the first reports in VA imaging were published. Both multiparametric top-line systems and portable or pocket-sized systems can be used
at bedside, operating, and hemodialysis rooms. Thus, the question is why US, now considered as the fifth pillar of physical semiotics, should not be systematically used in VA management.
This monothematic issue aims to update the role of the US in VA. It suggests the widespread use of Point-Of- Care Ultrasound (POCUS) with miniaturized, portable handheld devices using an imaging program in preopera- tive mapping, maturation period, and VA surveillance to avoid the major complications. In other words, it is time to add the insonation as the fifth pillar of the VA examination.
1Institute of Life sciences, Department of Internal Medicine, Sant’Anna School of Advanced Studies, University of Pisa, Pisa, Italy
2Nephrology Department, Parc Taulí University Hospital, Parc Taulí Research and Innovation Institute (I3PT), Autonomous University of Barcelona, Barcelona, Spain
3Center for Vascular Access, General University Hospital, First Faculty of Medicine, Charles University, Prague, Czech Republic
Corresponding author:
Meola Mario, Institute of Life sciences, Department of Internal Medicine, Sant’Anna School of Advanced Studies, University of Pisa, Via Roma 45, Pisa 56100, Italy.
Email: mario.meola@unipi.it